Better lucky than good?

The key to functioning well with heart disease is maintaining the heart’s ability to pump as much blood as needed. The best way to keep a heart attack from reducing that function is not to have one in the first place or at least have one that is very small. If that option is unavailable, then start with a heart that can pump more than is usually needed.
Control. Some, but not all, heart attacks are avoidable (see “Prevention” booklet). Unfortunately, the size of a heart attack is mostly beyond our control. Timely treatment (and one medicine) can reduce the size of a heart attack. However, the symptoms of a heart attack may pass without notice almost ½ of the time. Therefore, the factor over which we have the most control is maintaining the pump in the best possible shape to weather an event that we may not be able to prevent.
Conditioning
Fortune favors the prepared heart.
Muscles repeatedly forced to overcome a challenging weight or resistance become larger and thicker. Indeed, body builders rely on this gift of nature to sculpt their physique. The comparable adaptation of the heart that is most useful during severe illness is the ability to pump large quantities of blood on demand. At rest, the heart normally pumps just over a gallon of blood each minute. During effort, the heart’s output may briefly rise to over four gallons. A heart that is repeatedly asked to send out more blood during exercise will grow in size and capacity to easily accommodate its routine. Muscles in sustained activity require large volumes of blood for as long as the exercise is maintained. Therefore, endurance activities encourage the heart to grow and increase its capacity. The heart of an elite athlete is capable of extraordinary feats, sometimes capable of an output in excess of 10 gallons per minute.
Preparation for the challenges posed by coronary artery disease does not require the large heart of an elite athlete. Even the effect of moderate exercise produces valuable adaptation.
Coronary Arteries
Physical Activity
Walking is the physical activity for which we are designed, but any activity is beneficial for conditioning. I usually recommend a 10-15 minute walk, with a long-term goal of approaching 2 miles/30 minutes daily. Other activities are listed in the table below for comparison.
Making a bed
Doing dishes
Raking leaves
Snow Shoveling
Brisk walking (15 min/mile)
Golf (carrying clubs)
Doubles Tennis
Biking 5 mph
Hiking- light
Rowing 5 mph
Jogging. Rough estimate of
Mets= 100 divided by (min/mile)
Basketball
Stair climbing
*A metabolic equivalent (Met) is the amount of energy used by the body while at rest, under normal circumstances (about 2 kcal/lb per h).
Working with Angina pectoris
Medicines relieve symptoms to allow better conditioning.
Once coronary artery disease has shown its face and produced symptoms, the chance of having a heart attack is very real and the value of regular physical activity even greater. Unfortunately, angina may place a limit on exercise. Angina is produced when the work of the heart muscle exceeds its blood supply. Fortunately, the medicines listed in the table are very effective at easing the heart’s burden, improving its blood supply, or both to relieve symptoms. Relief of symptoms allows regular exercise to improve physical fitness. Efficient body muscle needs less blood to perform, thus further relieving symptoms. In fact, angina that significantly limits activity may be substantially relieved or completely resolve when the effects of conditioning add to the relief provided by medicines. The greatest value of relieved angina is to allow increased daily activity, increasing the heart’s capacity and making it more capable of facing future challenges from illness.
Atenolol
Propranolol
Bisoprolol
25-200 mg/d
120-240 mg/d
10 mg/d
Slow heart rate
Nightmare
Hairloss
Nasal Stuffiness
Nitroglycerin patch
Isosorbide
Mononitrate
5-10mg/d
30-120 mg/d
sublingual
low blood pressure
Channel
Antagonists
Amlodipine
2.5-10 mg/d
Leg Swelling
Low blood pressure
low heart rate (verapamil/diltiazem)
Antagonist
One type of medicine, the “Beta” blocker, not only reduces symptoms, but can also reduce the size of a heart attack. It protects the heart by blunting fear, anger and any stress response of the body that uses adrenalin to gain effect.
Surgery and Stents
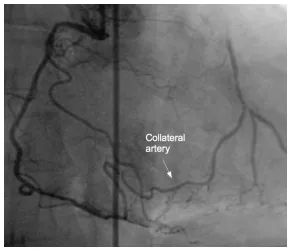
When the heart is called to pump more blood, it works faster and harder. For every extra heartbeat completed in a minute’s time, that much extra blood must be supplied to the muscle through the coronary arteries. A region of heart muscle fed through a diseased artery has an effective cap on the work that it can perform.
The cap is loosened by medicine and conditioning, but the process is slow. In the event that symptoms remain troublesome or when almost all heart muscle is dependent upon diseased arteries for its blood flow, surgery can make routes around the block and stent-angioplasty can just move the blockage out of the way. Symptoms are relieved immediately. In addition, properly fed muscle immediately increases its ability to pump blood and will improve even more with additional conditioning.
Coronary Bypass Surgery
The two ways to deal with a clogged pipe are to open it or just go around. The coronary arteries are small and have few long, straight segments. Surgeons can clean out the narrowed segments, but it is difficult and not particularly successful. Going around the diseased part of the artery works much better. That is called bypass surgery. Bypasses are made of veins or arteries. When veins are used, they are taken from other parts of the body. One end of the vein is attached so that it obtains blood from the large artery (Aorta) as it leaves the heart. The other end is attached to deliver blood beyond the narrowed point in the artery.
Arteries can also be used to create bypasses. The radial artery can be taken from the arm and used in the same fashion as a vein. An artery that is already present inside of the chest can be used as a bypass in a different way. Rather than taking it completely free of its moorings, its origin is left intact. With its other end taken free, it is essentially dangling free above the heart. The free end is attached to the coronary artery feeding the front and tip of the heart. This type of bypass has remarkable longevity, with more than 90% still working over 18 years after the surgical procedure.
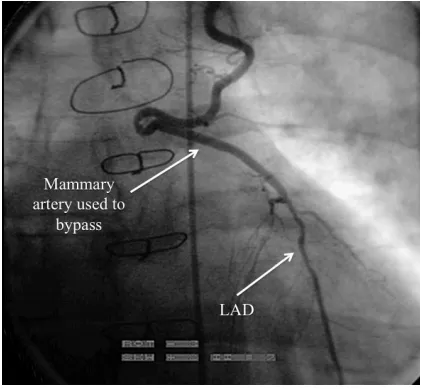
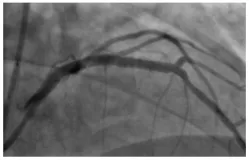
The LIMA is attached to the coronary artery to the front of the heart.
Stent-assisted Angioplasty
Angioplasty is performed through a catheter, without major surgery. A hair-thin wire is sent through the narrowed point in a coronary artery. A balloon-tipped catheter tracks along the wire, coming to rest at the narrowing. The balloon is designed to stretch only to a specific size. Inflation reshapes the narrowing to allow more blood to pass. The balloon and wire are then withdrawn.
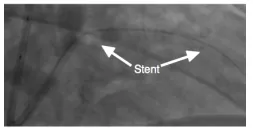
Stent. A stent is a metal cylinder whose paper-thin walls have had slits cut into them. The stent is placed on the outside of a balloon. 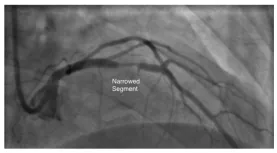
Who should have surgery or stentassisted angioplasty?
A surgery or stent procedure provides immediate relief from symptoms and improved function of the part of the heart whose blood flow has been restored. However, procedures have the potential for causing harm just in the attempt. The risk is small, but cannot be ignored. Most people can obtain reasonable relief from angina with medicines and physical conditioning, which are virtually risk free.
When symptoms remain unacceptable despite medicines and attempted conditioning, procedures offer an additional option for relief.
A hobbled heart may need a procedure.
The most important value of these procedures is to someone whose disease has already reduced pump function. Under these circumstances, conditioning may not be able to offer the best protection or be capable of providing it in a reasonable amount of time. The heart’s function is measured using exercise tests as well as motion pictures of the heart as it ejects blood. (see “Tests” booklet).
Conclusion
To survive a heart attack, have one that is small and have a heart capable of pumping large amounts of extra blood before the injury occurs. Since the size of a heart attack is mostly beyond our control, maintaining the pump, in preparation for illness, is our best option. Maintenance includes,
Conditioning: any activity, preferably something enjoyable, that asks extra work of the heart repeatedly. Walking is an excellent example.
Relief from angina that limits conditioning efforts. With time, the combination of conditioning and medicine may relieve most or all symptoms.
Angina, unrelieved by medicine, can be treated with coronary bypass surgery or stentassisted angioplasty. Both are very effective, but both are procedures that pose a risk of harm just in their performance.
Immediate improvement of function is also a benefit of surgery or stent treatment. This effect is sought when the heart’s function is severely impaired at the time a problem is recognized. The decision is guided by a number of heart tests and in-depth discussion with your physician.



