Dr. Wilson trained in General and Interventional Cardiology at St. Luke’s Episcopal Hospital/Texas Heart Institute. He worked for several years with the most respected physicians in Cardiology and Cardiac Surgery before becoming the director of the teaching program. While at THI, Dr. Wilson helped to begin the Cardiac-MRI diagnostic testing center, was the principle cardiologist involved in developing the STEMI program for treatment of Heart Attack and introduced routine Radial/Wrist access heart catheterization to the catheterization laboratory. He maintains his interest in Electrocardiogram interpretation and the Cardiac physical examination for diagnosis.
Dr. James Wilson is here to see that your health greatly improves with treatments for a variety of heart conditions. Houston MDs provides treatment for Angina, Atrial Fibrillation, Cardiomyopathy, Congestive Heart Failure, Heart Failure, Hypertension, and much more. Finding the right heart doctor is crucial because the condition of your heart is crucial. Our cardiologists have all the necessary education, training, and experience to provide the best medical treatment for your conditions.
If you are in the Houston, TX area looking for a heart doctor, rely on Houston MDs. We are proud to provide our patients with quality care and attention to detail. Please contact us today at 713-790-1775 or 832-336-1530.
Click Below To Learn More
Education
University: Louisiana Tech Univ., Ruston, LA 1986 Medical School: Tulane University School of Medicine, New Orleans, LA 1990. Residency: Internal Medicine, Baylor Coll. of Medicine, Houston, TX 1993 Fellowship: Cardiovascular Disease, Texas Heart Institute, Houston, TX 1997
Professional
General and Interventional Cardiology Established with Steven Neish: Joint Training Program for Adult Congenital Heart Disease at Texas Heart Institute/Texas Children’s Hospital Originating Co-Director Cardiovascular MRI St. Luke’s Episcopal Hospital Key Cardiology Physician creating the St. Luke’s Episcopal Hospital STEMI program Initiated and Maintain Heartsounds Lab teaching website, www.heartsounds.com
Academic Appointments
Robert J. Hall Chair of Cardiovascular Disease 2008-2016 Director of Cardiology Education, SLEH/Texas Heart Institute 2003-2016 Professional Staff Texas Heart Institute 1997-2016
Honors and Awards
Lambda Sigma Honor Society Alpha Epsilon Delta Pre Medical Honor Society Phi Kappa Phi Honor Society Alpha Omega Alpha Medical Honor Society Paracelsus Award for excellence in Toxicology John Taylor Halsey Award for excellence in Pharmacology Chief Medical Resident for St. Luke's Episcopal Hospital 1994 Chief Cardiology Fellow 1996 Outstanding Cardiology Fellow 1997 Resident Teaching Award, Baylor College of Medicine 1999-2003, 2007-2014 Robert J. Hall Teaching Award – 2007
Board Certification
National Board (Part I) National Board (Part II) Federal Licensing Examination American Board of Internal Medicine Cardiovascular Disease 1998, 2007, 2017 Certificate of Added Qualification for Interventional Cardiology 1999
Other non-academic positions
Chief of Staff St. Luke’s Episcopal Hospital (2014-15) Director Clinical Cardiovascular Services St. Luke’s Medical Center 2006-10 Clinical Chief Cardiology St. Luke’s Episcopal Hospital 2010-2016 Director Heart Sounds Laboratory Texas Heart Institute 2007-2016
National Scientific Participation
Journal Editorial Boards Editorial Board: Texas Heart Institute Journal Clinical and Applied Thrombosis/Hemostasis
Reviewer: Circulation Catheterization and Cardiovascular Cardiology Journal of Electrocardiography Yonsei Medical Journal
Professional Societies
Texas Heart Institute Cardiac Society 1997-2016 Member-at-Large 1998 Vice President 1999 President 2000
American College of Cardiology Fellow Counselor – Texas Chapter 2003 - 2012 American College of Physicians- Member International Academy of Clinical and Applied Thrombosis/Hemostasis
This blog is intended to inform and teach about Cardiology. It includes comments and opinions about procedures but is intended only for educational purposes. We cannot be held liable for its content and is not intended as a how-to manual.
Currently about 10% of people in the US have catheterization done using the wrist as opposed to over 70% in other parts of the world. Dr. Wilson has performed over 500 such procedures and uses the wrist 90% of the time, including for angioplasty and stent placement.
What is Heart Catheterization?
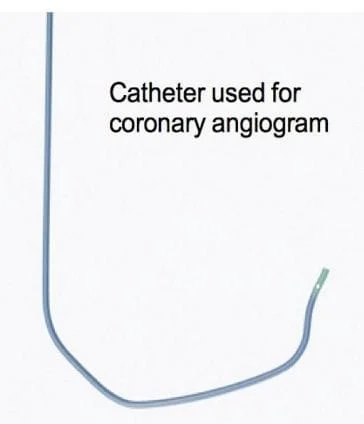
Almost 1/3 of people in the US will encounter some form of heart or artery disease in their lives. Heart attack and limiting chest discomfort are often due to disease of the arteries that feed the heart. In order to diagnose and treat these problems, heart catheterization, which includes taking pictures of the arteries, is often necessary. A catheter is simply a long tube that may be manipulated to points inside of the body without a full, open surgical procedure. In many instances, the location of the coronary artery that is the source of limitation or discomfort can be identified and corrected through a catheter. Heart catheterization is performed on thousands of people every day.
Why the wrist?
Catheters that will be steered to the heart traditionally entered the body through the artery in the groin. The catheters were large and the groin artery (femoral) is large enough to accommodate them. Catheters and tools used to correct some artery problems are smaller today. As a result, the artery in the wrist (radial) may be used instead of the groin.
The chance of bleeding is lower with the wrist compared to the groin.
The wrist is easy to examine and does not require any period of bedrest after the procedure.
Most people find the wrist procedure more comfortable.
Can Everyone Have Radial Artery Catheterization?
About 5% of people have anatomy that prevents catheterization through the wrist. The radial artery of 1-2% of people makes twists and turns that won't allow a catheter. However, the most common limitation remains the size of catheters. In some of us, the radial artery is just too small to accommodate even the smallest catheters. In addition, there must be good blood supply to the hand through both of the radial and ulnar arteries of the wrist. Prior to wrist catheterization, the blood supply to the hand is examined closely and the radial artery is measured using ultrasound. If you would like to learn more about radial cardiac catheterization for yourself, please contact us.
What is a Heart Attack?
Today, we know heart attack as an illness with a well-defined cause, course and potential treatment. Before modern medicine, the understanding was quite different.
In medical school, I asked one of my instructors what a heart attack was. He told me it was a fit of chest discomfort that left you sick for months, if you survived. In error, I took this as a dismissal, something along the lines of, “Go away kid. You bother me.” The truth was that he had simply restated an original understanding of the illness. Before the tools of modern medicine peaked inside of the body, all that was known of any illness was the type of discomfort that it caused, how you might have picked it up (liberal eating habits or being around other sick people) and what came with it, like fever, rash or cough. Before it was called heart attack, these events were a day or so of ill-defined chest discomfort followed by profound illness whose cause was unknown.
The first glimmer of an illness
Chest discomfort was long recognized as a sign of danger but only as a part of other illnesses.
Physicians of the ancient world made mention of chest discomfort as a potentially threatening complaint, but not in great detail. Infections, starvation/malnutrition, and injury were the dominant threats to wellbeing. Physicians were busy with hygiene and good nutrition. Some chest discomfort that was troubling mostly older, fatter people failed to garner much interest. By the 18th Century, the problem had grown and a physician named Heberden felt it should be recognized. He saw a pattern in the type of discomfort, who was affected and the severe illness that came with it. In a description, provided so that all physicians could recognize the warning, Heberden gave this illness a name, Angina pectoris . The name described, not pain, but a strangling or anguish inside of the chest. He had no idea what caused this discomfort, only that the illness was disabling and sometimes fatal.
Angina pectoris
Angina may be just a little different for everyone
The most common description is a burning, boring or pressure-like discomfort, usually felt in the center of the chest.
Angina is a symptom. It is a sensation that the body uses to send a warning of trouble within.
Many heart attack survivors look back on events and realize that they missed warning signs of what was to come because they thought that something so dangerous would hurt more. Although some survivors do report having felt pain, just as many people take pains to emphasize that what they felt was uncomfortable rather than painful.
Early on, discomfort is usually brought on by emotional stress or exercise and may also be felt in the upper back, neck, arms or jaw. With discomfort, many people notice shortness of breath, nausea, sweating and an anxiety that compels stillness or cessation of any offending activity.
Fatigue and Shortness of breath
Most disease of the heart is not truly felt by the heart. Rather, the heart’s impaired performance is made known through general sensations of fatigue or hunger for air. Fatigue in particular may be long-standing before angina appears or any disease of the heart is actually discovered.
Relief
Angina is relieved by rest or nitroglycerin, with typical episodes resolving slowly, over 1-30 minutes.
ATTACK
Once angina has appeared, its threat looms. Exceed the boundary placed on physical activity, fear, anger or worry and angina will return. Symptoms might occur even earlier after a meal or in cold wind. Meanwhile, symptoms resolve slowly after ceasing the offending activity. The propensity for angina to pounce at any offense and recede slowly in a lingering reminder of its inevitable return made many people refer to symptoms as “attacks”.
The cause of angina: the heart
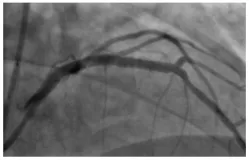
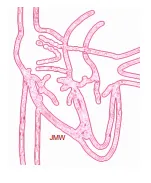
Angina is the language that heart muscle uses to communicate with the brain. It sends a warning, but the warning lacks clarity. When the hand hurts, the mind knows of the hand. When the heart hurts, the mind knows only that something is wrong, not what. The sensation arises when heart muscle has to use more energy than it is given. Therefore, angina may arise from an overworked heart. However, the most common cause is decay of the arteries that deliver blood/energy to the heart. The decay is called atherosclerosis or coronary artery disease.
Angiogram of a diseased coronary artery
Heart Attack
Atherosclerosis is unpredictable. The disease may worsen suddenly. If so, angina appears without provocation. No exercise. No worries. Just angina. The sensation may also be more intense or last longer than the typical 1-30 minutes. These attacks of angina stand out because they are a change. New onset symptoms, a changing pattern, or intensity is often a sign of imminent danger. Even if a severe bout of discomfort resolves, fortunate survivors might be left with crippling fatigue or difficulty breathing. Historically, these most severe attacks of angina merited the singular designation of “A Heart Attack”. We still know them as such, but understand the cause much better.
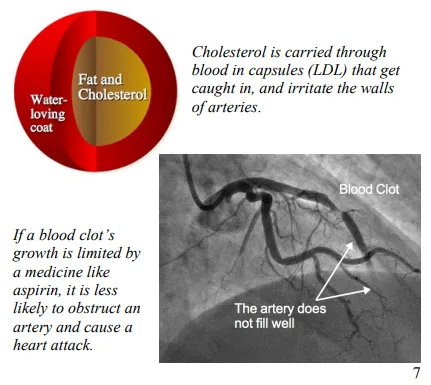
What happens?
Diseased arteries may cause blood to clot at any time. Clots are unpredictable and can grow or change quickly. As the clot grows larger, there is less room for blood to pass to heart muscle. The result is new onset or changing symptoms. If the artery closes, damage to heart muscle–a heart attack–occurs.
How can I tell?
Risk Factors for Heart Attack
Age
Smoking
Diabetes
Obesity
High blood pressure
High Cholesterol
Chronic Kidney
Disease
HIV infection
Angina is known by the company that it keeps.
The heart is not the only source of dull discomfort in the chest. However, the heart should be assumed to be the source of unexplained symptoms in anyone who also has risk factors for developing disease of the arteries. The most important risk factor is age. The most dangerous are smoking and diabetes mellitus. An example of how risk factors are used follows. In a 20-year-old woman who complains of chest discomfort after eating a hot dog covered in mustard, the absence of any risk factor and her culinary tastes point to acid reflux as the likely 11 source of her symptoms. Were she 45 years of age, with a cigarette habit or troubled by high blood pressure the same sensation is not so easily dismissed, even if the hot dog and mustard are still part of the story.
What to do
Should you recognize discomfort that might be angina, discussion with your doctor or healthcare provider is urgent. A dispassionate observer can better evaluate the meaning of symptoms and context to decide if more investigation or treatment is needed. New or progressive symptoms may be a warning of trouble to come. Modern medicine offers a rescue from trouble, if it is caught in time.
Call for Help.
When faced with a persistent discomfort that you are concerned may be coming from your heart, the most important first step is to ask for help. Tell someone nearby, contact a professional or call 911.
What I offer
Rescue
Evaluate new or changing symptoms to identify warning signs for heart attack and stop the process.
INTERVIEW/EXAM/EKG HOSPITAL CARE TESTING
Echo/Stress/CT Testing through hospital based laboratories.
Heart Catheterization, when necessary, to visualize the coronary arteries: mostly done through the wrist.
TREATMENT
Address the problem artery with medicines and other treatments if needed.
An artery caused symptoms that were threatening.
The same artery after repair
Preparation
Improving overall health to enjoy life and withstand future challenges from heart attack or other illnesses.
Exercise
Maintaining fitness helps face any health challenge
Medicine
Provides relief from symptoms and protection for the future
Repair
Angioplasty or surgery to relieve the most severe symptoms or life threatening disease
Prevention
Address the underlying causes of arterial disease to avoid heart attack and stroke.
Lifestyle
Diet and exercise habits are the core focus of reducing risk. Most important are smoking cessation and controlling body composition
Medicine
Diabetes, high cholesterol and high blood pressure are, metabolic and functional derangements that affect arteries. Where control with diet and lifestyle alone is not possible, medicines such as aspirin and those for cholesterol lowering, glucose and blood pressure control can be invaluable.
Blood Pressure
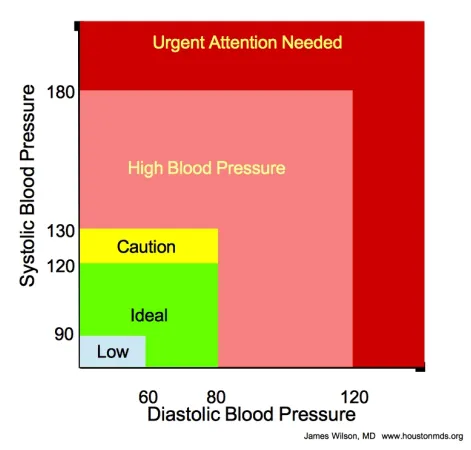
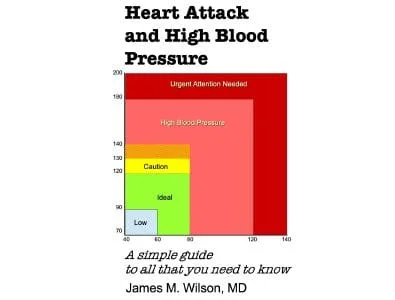
What the numbers mean, how to know if you’re normal and what to do if you’re not
What is High?
The current blood pressure recommendations are shown on the booklet cover. How we got there is quite a story and helps to understand the how and why that go with the recommendation.
When looking for guidance on the normal values for blood pressure, confusion reigns. Elephants lumber with a blood pressure of 190/120. The head sitting high above a giraffe heart asks a blood pressure of 235/160 to be fed properly. A frog rests quietly with a blood pressure of 40/20, while the rat and the rabbit hover near 120/80. Nature maintains blood pressure in a narrow range to ensure proper blood flow to the brain, the heart and everything else. Which narrow range depends upon the animal and the environment that shaped it. Ironically, the ideal range for us (see cover) was suggested when routine blood pressure measurement was first introduced. However, proving that the suggestion was a good one took quite some time and an enormous amount of effort.
By the way, these numbers aren’t lb/in2 like your car tires. The values are in millimeters of mercury.
In the beginning…
No one knows when high blood pressure first appeared. However, its complications have been around as long as written history.
At a time when people were living from meal to meal instead of paycheck to paycheck, blood pressure was unlikely to have been a major health problem. More pressing concerns were fevers, starvation, and tigers. Later, as accumulated learning and civilization brought longer lives and regular meals, the complications of high blood pressure began to register among physicians. Blood pressure may deviate from its natural settings for a number of reasons: heredity, hormones and kidney function. However, in most of us, it begins with salt intake, excess body weight and too little exercise. As diets began to change, with the liberal use of salt as a food preservative, blood pressure probably grew in importance. It grew silently because blood pressure cannot be felt or seen. It is not disfiguring. Its presence is known only when measured. Until about 200 years ago, no one measured. Widespread measurement of blood pressure truly began at the dawn of the 20th Century.
The complications
High blood pressure urges heart muscle to thicken, just as the muscle in the arm does when it is forced to lift weight repeatedly. Artery walls also grow thicker. These adaptations are provisions of nature to overcome challenges normally imposed by physical activity. Under the constant influence of abnormal blood pressure, adaptations become entrenched and cause disease. Thick heart muscle becomes stiff and inefficient. The thickened arteries lose their rubbery quality and offer resistance to blood movement. Abnormal arteries disrupt blood supply to parts of the kidney and brain.
Heart muscle and artery walls get thicker and stiffer. Everything happens in silence.
The laboring heart and failing kidney produce fatigue, difficulty breathing and fluid retention, historically referred to as “dropsy”. Meanwhile, arteries that fail to thicken under the load may stretch, enlarge and rupture. Rupture of an artery in the brain produces an illness known in the past as “apoplexy”. Today, we know these problems as heart failure, kidney failure, and stroke.
Mercury and measuring pressure
Before there were gauges and computers, the idea of pressure was referred to by the weight of a fluid or how high it stood in a container. Water is the ubiquitous liquid, but for experiments with different pressures, very tall containers of water were necessary.
A pressure of 2 lb/in2 is 100 mmHg
Elemental mercury is normally a fluid. It is also very heavy (14X water). Therefore, a tube filled to some specific level of mercury represents the same weight or pressure as a much larger tube filled with water. This made measurements much more convenient. Modern gauges can relate pressure in different ways. Your tire gauge is in PSI (lb/in2 ). However, the height of a column of mercury is still used to describe blood pressure.
Blood Pressure
Blood pressure is most easily measured by recording how hard we have to press on an artery to force it shut. The current technique uses a cloth belt, into which an inflatable bladder is sewn. 7 The belt is wrapped around a limb, with the bladder positioned over an artery. With the belt held tightly, the bladder is inflated to the point at which the pulse disappears. To measure pressure, the bladder is attached to a column of mercury in glass tubing. The rise of mercury is the pressure being applied to the artery.
Modern devices use a gauge rather than the mercury filled tube, but the markings are listed as millimeters of mercury. In addition, a stethoscope is used to listen to the artery, rather than feeling the pulse.
Systolic and Diastolic measurements
When the heart beats (systole), pressure in the artery briefly rises. When the heart rests (diastole), pressure falls to its lowest value. Using a stethoscope held just beyond the belt and over the part of the limb where the artery runs, the sound of each heartbeat can be heard from the artery during deflation of the bladder.
As the pressure in the bladder is reduced, a sound first appears when systolic blood pressure overcomes the compression from the bladder. The sound disappears when the compression from the bladder falls below the least (diastolic) pressure in the artery.
Standards
Blood pressure is typically measured in the upper arm, in the seated position.
Measurement should follow a 5-10 minute period of rest.
The bladder used in the belt (colloquially known as a cuff) should be at least 5 ½ inches wide and cover ½ the circumference of the arm.
Although not presently a standard, a two-week average of recordings taken at home, with an automated device, may be a more accurate reflection of blood pressure than those taken in the office setting.
Chasing Normal
After blood pressure measurement became commonplace, the values in young, healthy adults were used to get an idea of normal values. However, a child’s blood pressure is quite low, 80-90 mmHg and the young adult’s slightly higher at about 100- 110. Older, healthy people had pressures that were even higher still. Therefore, many people felt that “normal” had a wide range and that blood pressure probably increases, as we grow older.
The first population studies of blood pressure came from insurance companies in the early 1900’s!
Statistics . Life insurance companies quickly realized the value of blood pressure measurement as a tool to uncover hidden risk. Two companies applied some recently developed mathematical techniques to provide the first scientifically derived estimate of normal blood pressure. To do so, they examined the blood pressure of in large numbers of normal people. They also compared pressure at enrollment to later health status. The results suggested normal to be a systolic value in the 120’s and not more than 140. A blood pressure over 150 warned that the individual who appeared normal today, might not stay that way for very long.
Blood pressure has since been examined exhaustively from the perspective of age, body habitus, diet, habits and heritage. In addition, illnesses that develop over time have been correlated to the first blood pressure, its change over time, and with the context of additional problems like diabetes mellitus or smoking.
Normal Blood Pressure is <120/80 mmHg
Any person whose blood pressure is consistently above 120/80 faces a chance of illness in the future that is higher than another, otherwise identical, person whose blood pressure remains lower. The relationship is seen most easily with stroke. However, high blood pressure also affects the development of heart failure, kidney disease and heart attack.
Treatment
Lifestyle
Moderate calorie restriction, monitored sodium and minimal alcohol intake, along with regular exercise are called a “healthy lifestyle”.
LESS BODY FAT MORE MUSCLE <2000 MG SODIUM/DAY
Anyone concerned about the eventual development of cardiovascular disease can follow the recommendations of healthy lifestyle without risk of harm and with full expectation of benefit. The potential gain makes the recommendation all the more urgent when blood pressure is consistently above normal, 120/80 mmHg
MEDICINE
The menu of medicines that lower blood pressure is extensive, allowing attempts to steer blood pressure to a desired range, with the least chance of unwanted effects
Medicines alter blood pressure by:
Relaxing tiny arteries
Manipulating or blocking hormone effects
Blunting the communication of nerves that influence blood pressure.
Encouraging the kidney to release sodium.
Excess blood pressure lowering may produce fatigue, lightheadedness, confusion or poor balance
The potential for medicines to cause unintended side effects required that the relationship of blood pressure and its complications be revisited during medical care in order to define when the illness was more dangerous than the intended treatment. A threshold of 140/90 is the point at which medical treatment of blood pressure is consistently valuable .
Meanwhile, diabetes, high cholesterol, and smoking contribute to the same diseases caused by high blood pressure. People who have an illness or behavior posing a threat to their health, in addition to abnormal blood pressure, gain from medical treatment beginning at values in excess of 130/80.
Treat blood pressure above 130/80 if you have diabetes
Which Medicine?
Some medications can address more than one illness at the same time. Thus, the presence of any of these additional illnesses often drives the choice of medicine. Absent that, whatever medicine works best, with the least side effects is a good choice.
What is the goal blood pressure?
If you are not taking medicine, but paying attention to your blood pressure and lifestyle, the goal is an average blood pressure <120/80.
Medicine?
Since medicine can occasionally overcorrect, the goals of blood pressure during treatment are different than those with diet/lifestyle. Generally, the goal is to reduce the blood pressure to below the threshold value that prompted treatment. If you started because of a blood pressure above 130/80 in the presence of another illness, then that is the goal. It probably should be the same for everyone, but without additional illnesses, <140/90 is acceptable.
<140/90 is OK <130/80 is GOOD
But I can’t tolerate that blood pressure!
In older people and those with high blood pressure for a long time, blood pressure may need to be lowered slowly to avoid side effects. Therefore, goals are individualized with the help of a physician. Some societies recommend an initial goal of <160/90 for older people, with longstanding high blood pressure, who are beginning treatment.
Conclusion
Ideal blood pressure is shown on the COVER as the GREEN ZONE. A consistent diastolic blood pressure over 80 warrants a discussion with your physician and consideration for treatment. For systolic values,
120-130 is acceptable, but should make you take notice and attend to diet and exercise.
130-140 is high blood pressure. The decision to take medicine requires consideration of additional health risks.
140 , treatment is almost certainly necessary. While taking a medicine to control blood pressure, <130/80 is the acceptable, or treated normal value. To assist your physician, obtain an automated device that you can use at home. Take values after 5-10 min of rest, at scheduled times once or twice daily and record them. The 2-week average is an important number.
The caveat to all of these recommendations is that
The first focus of attention to blood pressure is lifestyle: diet, exercise, weight management and minimal alcohol intake.
Recommendations are not rules, but points for discussion with your physician.
Better lucky than good?
By some estimates, 50% of the time that heart muscle is damaged, it goes unrecognized.
The key to functioning well with heart disease is maintaining the heart’s ability to pump as much blood as needed. The best way to keep a heart attack from reducing that function is not to have one in the first place or at least have one that is very small. If that option is unavailable, then start with a heart that can pump more than is usually needed.
Control. Some, but not all, heart attacks are avoidable (see “Prevention” booklet). Unfortunately, the size of a heart attack is mostly beyond our control. Timely treatment (and one medicine) can reduce the size of a heart attack. However, the symptoms of a heart attack may pass without notice almost ½ of the time. Therefore, the factor over which we have the most control is maintaining the pump in the best possible shape to weather an event that we may not be able to prevent.
Conditioning
Fortune favors the prepared heart.
Muscles repeatedly forced to overcome a challenging weight or resistance become larger and thicker. Indeed, body builders rely on this gift of nature to sculpt their physique. The comparable adaptation of the heart that is most useful during severe illness is the ability to pump large quantities of blood on demand. At rest, the heart normally pumps just over a gallon of blood each minute. During effort, the heart’s output may briefly rise to over four gallons. A heart that is repeatedly asked to send out more blood during exercise will grow in size and capacity to easily accommodate its routine. Muscles in sustained activity require large volumes of blood for as long as the exercise is maintained. Therefore, endurance activities encourage the heart to grow and increase its capacity. The heart of an elite athlete is capable of extraordinary feats, sometimes capable of an output in excess of 10 gallons per minute.
Preparation for the challenges posed by coronary artery disease does not require the large heart of an elite athlete. Even the effect of moderate exercise produces valuable adaptation.
Coronary Arteries
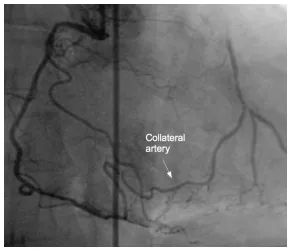
A second effect of conditioning is important when disease has already changed the arteries that feed the heart. Three coronary arteries feed the heart, each with very small connections to the others. These small connections are not typically in use. When the heart pumps more blood, it needs more blood delivered through the coronary arteries. When a narrowing is present, the increased need for blood flow to heart muscle enlists these extra connections to provide an alternate route for blood to get to heart muscle. Extra connections can grow to a size that almost replaces the function of the original artery.
Physical Activity
Walking is the physical activity for which we are designed, but any activity is beneficial for conditioning. I usually recommend a 10-15 minute walk, with a long-term goal of approaching 2 miles/30 minutes daily. Other activities are listed in the table below for comparison.
Biking 20 mph Rowing 5 mph Jogging. Rough estimate of Mets= 100 divided by (min/mile) Basketball Stair climbing
*A metabolic equivalent (Met) is the amount of energy used by the body while at rest, under normal circumstances (about 2 kcal/lb per h).
Working with Angina pectoris
Medicines relieve symptoms to allow better conditioning.
Once coronary artery disease has shown its face and produced symptoms, the chance of having a heart attack is very real and the value of regular physical activity even greater. Unfortunately, angina may place a limit on exercise. Angina is produced when the work of the heart muscle exceeds its blood supply. Fortunately, the medicines listed in the table are very effective at easing the heart’s burden, improving its blood supply, or both to relieve symptoms. Relief of symptoms allows regular exercise to improve physical fitness. Efficient body muscle needs less blood to perform, thus further relieving symptoms. In fact, angina that significantly limits activity may be substantially relieved or completely resolve when the effects of conditioning add to the relief provided by medicines. The greatest value of relieved angina is to allow increased daily activity, increasing the heart’s capacity and making it more capable of facing future challenges from illness.
Headache,Constipation Leg Swelling Low blood pressure low heart rate (verapamil/diltiazem)
Multi-channel Antagonist
Ranolazine
500-1000 mg 2/d
Tremor, Long QT
One type of medicine, the “Beta” blocker, not only reduces symptoms, but can also reduce the size of a heart attack. It protects the heart by blunting fear, anger and any stress response of the body that uses adrenalin to gain effect.
Surgery and Stents
When the heart is called to pump more blood, it works faster and harder. For every extra heartbeat completed in a minute’s time, that much extra blood must be supplied to the muscle through the coronary arteries. A region of heart muscle fed through a diseased artery has an effective cap on the work that it can perform.
The cap is loosened by medicine and conditioning, but the process is slow. In the event that symptoms remain troublesome or when almost all heart muscle is dependent upon diseased arteries for its blood flow, surgery can make routes around the block and stent-angioplasty can just move the blockage out of the way. Symptoms are relieved immediately. In addition, properly fed muscle immediately increases its ability to pump blood and will improve even more with additional conditioning.
Coronary Bypass Surgery
The two ways to deal with a clogged pipe are to open it or just go around. The coronary arteries are small and have few long, straight segments. Surgeons can clean out the narrowed segments, but it is difficult and not particularly successful. Going around the diseased part of the artery works much better. That is called bypass surgery. Bypasses are made of veins or arteries. When veins are used, they are taken from other parts of the body. One end of the vein is attached so that it obtains blood from the large artery (Aorta) as it leaves the heart. The other end is attached to deliver blood beyond the narrowed point in the artery.
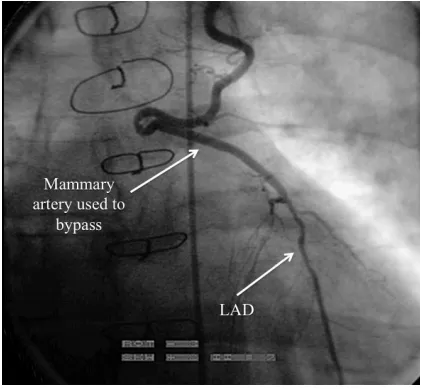
Arteries can also be used to create bypasses. The radial artery can be taken from the arm and used in the same fashion as a vein. An artery that is already present inside of the chest can be used as a bypass in a different way. Rather than taking it completely free of its moorings, its origin is left intact. With its other end taken free, it is essentially dangling free above the heart. The free end is attached to the coronary artery feeding the front and tip of the heart. This type of bypass has remarkable longevity, with more than 90% still working over 18 years after the surgical procedure.
The LIMA is attached to the coronary artery to the front of the heart.
Stent-assisted Angioplasty
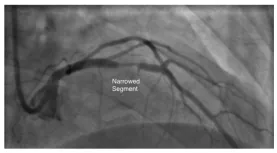
Angioplasty is performed through a catheter, without major surgery. A hair-thin wire is sent through the narrowed point in a coronary artery. A balloon-tipped catheter tracks along the wire, coming to rest at the narrowing. The balloon is designed to stretch only to a specific size. Inflation reshapes the narrowing to allow more blood to pass. The balloon and wire are then withdrawn.
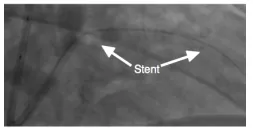
Stent. A stent is a metal cylinder whose paper-thin walls have had slits cut into them. The stent is placed on the outside of a balloon. With inflation of the balloon, the slits open further and the metal bends like an accordion gate. The bent parts of the former cylinder become a meshwork of struts that support the walls of the artery in its new shape.
The balloon is deflated and removed. The artery heals over 3-12 months. Drug-Eluting stents use medicines to control the healing process inside of the treated coronary artery. This reduces the chance that a narrowing can reform during that first year. After stent-assisted angioplasty, the clotting system must be rigorously controlled with medication for the 3- 12 month healing period.
Who should have surgery or stentassisted angioplasty?
A surgery or stent procedure provides immediate relief from symptoms and improved function of the part of the heart whose blood flow has been restored. However, procedures have the potential for causing harm just in the attempt. The risk is small, but cannot be ignored. Most people can obtain reasonable relief from angina with medicines and physical conditioning, which are virtually risk free.
When symptoms remain unacceptable despite medicines and attempted conditioning, procedures offer an additional option for relief.
A hobbled heart may need a procedure.
The most important value of these procedures is to someone whose disease has already reduced pump function. Under these circumstances, conditioning may not be able to offer the best protection or be capable of providing it in a reasonable amount of time. The heart’s function is measured using exercise tests as well as motion pictures of the heart as it ejects blood. (see “Tests” booklet).
Conclusion
To survive a heart attack, have one that is small and have a heart capable of pumping large amounts of extra blood before the injury occurs. Since the size of a heart attack is mostly beyond our control, maintaining the pump, in preparation for illness, is our best option. Maintenance includes,
Conditioning: any activity, preferably something enjoyable, that asks extra work of the heart repeatedly. Walking is an excellent example.
Relief from angina that limits conditioning efforts. With time, the combination of conditioning and medicine may relieve most or all symptoms.
Angina, unrelieved by medicine , can be treated with coronary bypass surgery or stentassisted angioplasty. Both are very effective, but both are procedures that pose a risk of harm just in their performance.
Immediate improvement of function is also a benefit of surgery or stent treatment. This effect is sought when the heart’s function is severely impaired at the time a problem is recognized. The decision is guided by a number of heart tests and in-depth discussion with your physician.
Preventing heart attack
Within 5-years of a heart attack, 20-45% of people will have another complication of their disease. Therefore, the tools to prevent the first heart attack are even more important after the first heart attack.
The Healthy Lifestyle
Restrict Calories (address their source secondarily)
Exercise regularly
Avoid smoking
The keys to prevention are in identifying our own traits or behaviors that hasten arterial decay. Some are obvious, like overeating and smoking. Others depend upon tests of metabolism and things that we are unable to see or feel until its too late.
Corrective efforts range from simple and risk free to complex. Simple efforts are part of a healthy lifestyle. Complex efforts employ medicines to control what lifestyle cannot. Medicines that control diabetes mellitus and blood pressure, lower LDL cholesterol and reduce the chance of blood clotting have an enormous impact on the chance heart attack.
Diabetes
Diabetes mellitus (DM) is more complicated than blood sugar. One type of DM develops after the body stops making insulin. It is most common in young people and is treated with replacement of insulin. Non-insulin requiring, Type II or Adult Onset DM is actually a collection of metabolic problems with impaired response to insulin in common. Elevated blood sugar is the most easily recognized and dangerous part of the disease. However, managing blood sugar is only one part of addressing the disease.
There is more to diabetes than blood glucose
Adding extra insulin on top of what the body makes helps to control glucose, but does not correct the underlying problem. The goal is to restore the body’s sensitivity to insulin, primarily through diet, exercise and reducing body fat. Medicines like Metformin can reduce the need for insulin. The choice of medicines used for control must be tailored to you and is a rapidly changing field. Therefore, regular review of the value of individual medicines with a primary physician or diabetes specialist is an extremely important measure to prevent heart attack.
Obesity
We need muscle. Aside from locomotion, muscle uses energy and helps to control the amount of fat and sugar in blood. Fat, on the other hand, was intended as the small reserve for times of need. Fat speaks. It has a personality opposite muscle, urging the blood content of fat and sugar to rise. Excess body fat residing in the belly is most dangerous.
A man’s waist size >35 in. or a woman’s >40 may mean trouble.
The goal is to keep the amount of fat controlled without losing muscle. Weight loss driven by strict calorie restriction takes from both fat and muscle. Any weight that returns is usually fat. The net result of weight that swings down and up is less muscle in comparison to fat. Reduce the waistline with diet and exercise to maintain muscle and keep at it to avoid swings.
Exercise
Regular activity improves sleep, lessens joint pain from mild or moderate arthritis, and confers an overall sense of wellbeing. The exercise for this purpose uses large muscle groups in moderate activity for 20-30 minutes each day . Specific activities and their energy expenditures are provided in booklet 3, “ Preparation for the unexpected ”.
Diet
Swing a stick and you’ll probably hit a diet. With so many different options, the basic idea sometimes gets lost in details. With respect to heart disease, the KEY POINTS are:
The first major focus of your diet is the number of calories taken each day.
Adding “healthy” food to a full diet is rarely useful if nothing is removed. A healthy change means a substitution rather than an addition.
If you are taking medicine or being treated for other illnesses, consultation with a dietician is invaluable.
Normal nutritional needs must be met, including essential fat, protein, vitamins, and minerals. Many are available in pill form, but food is better and cheaper.
Limit intake of saturated fat (fat that is solid at room temperature, usually found in meat and dairy) as much as possible. Limit sodium intake to 1-2000 mg/d.
A diet is not torture. Find a way to make it enjoyable and, every once in a while, take a day off and enjoy something on the forbidden list, if this can be done safely
An easy first step in calorie reduction is to follow the BRPP plan. That is to avoid bread, rice, potatoes, and pasta.
Smoking
Don’t. There is no magic here. It is incredibly hard to stop smoking. Nicotine supplements help, as do a few medicines. Talk to your doctor and find what works best for you. Just stop.
Medicines that prevent heart attack
In addition to medicines that treat diabetes, two types of medicine decrease the chance of having a heart attack: those that reduce LDL content in blood and those that retard blood clotting.
Lowering LDL . LDL transports cholesterol and triglyceride in blood. It is like a small sac that briefly allows oil and water to mingle. It is also the primary irritant of arteries, promoting CAD. Medicines that slow cholesterol production are our most effective option for reducing the number of LDL capsules in circulation.
Purpose
Drug
Effect
Dose/Target
Commment
Slow clotting
Aspirin Clopidogrel Prasugrel Ticagrelor
Platelet-inhibitor Platelet-inhibitor
75-150mg/d
Stomach bleeding indigestion asthma (rare) Consult with physician
The average calculated LDL-cholesterol concentration in US citizens is about 120-130 mg/dl. The value that appears to confer the lowest risk for heart attack is well below 100 and probably less than 50 mg/dl.
Oral medicines called Statins lock up the assembly line for cholesterol production. Less cholesterol is made inside of the liver cell, prompting a recall of the LDL in circulation. As a rule, a 20-30% decrease in LDL-cholesterol is necessary to reduce the chance of a heart attack. The main limitation with statin type drugs is that between 5-15% of people develop muscle discomfort as an intolerable side effect.
LDL gets back into the liver through a special window. PCSK-9 inhibitors (Proprotein convertase subtilisin/kexin type 9) hold that window open and decrease the amount of LDL in the blood well in excess of the 20-30% threshold. They can only be given by injection, but are very useful when a statin is insufficient.
Blood Clotting. Aspirin and other anti-platelet drugs are the most effective means of slowing blood clotting under conditions where blood flow is fast, like in arteries. Stunning platelets does not prevent artery walls from becoming irritated and angry, but limiting the size of a blood clot that forms in an angry artery definitely prevents heart attack.
Influenza Vaccine . Influenza troubles people with heart disease in two ways. Like any infection, it makes the heart work harder during the battle to recover. In addition, multiple effects of the virus can actually cause changes in arteries, promote blood clotting and trigger a heart attack.
Although medicines can help after the infection has begun, the most effective protection from the harms of influenza is a vaccine to prevent infection. Influenza is a master of disguise that changes its face to evade immunity. Therefore, we can suffer from influenza repeatedly. A new vaccine is made each year to match the face that the virus has chosen. Anyone with coronary artery disease or at very high risk for its presence should strongly consider getting the influenza vaccine on a yearly basis.
Angiotensin Converting Enzyme (ACE) is a key point in the network controlling blood pressure, kidney and heart function. ACE-inhibitors are a group of medicines that lower blood pressure, protect kidneys, and benefit people with heart disease unrelated to coronary artery disease. After a heart attack, ACEinhibitors protect the heart as it heals. Blood pressure control is crucial to avoiding heart disease. In people with coronary artery disease and in those at high risk for its development, ACE-inhibitors also reduce the risk of heart attack.
Alternative Medicines
Supplements for LDL reduction
The statins are the only oral medicine that can lower LDL effectively enough alone to lower the risk of heart attack. Several other types of medicine also influence LDL. They are not particularly effective alone but may serve as helpful additions to the statins.
Statins prevent cholesterol from being made. Another medicine called a Resin prevents cholesterol from being recycled. The liver uses cholesterol to make a detergent called bile. When a fatty meal gets to the intestine, the gall bladder dumps in bile to help with absorption of the fat. The intestine absorbs fat and the bile is recycled. Resins stick to the cholesterol component of bile to keep it from being recycled. The liver is forced to use its cholesterol to make bile and recalls LDL from the blood.
Ezetimibe is a synthetic inhibitor of cholesterol absorption in the intestine with an impact similar to the effect of resins.
Niacin is a B-vitamin that convinces the liver to make less of the fat carrying capsules that become LDL in blood. Niacin increases acid production in the stomach, causes terrible flushing and worsens gout. Its place in treatment is very limited.
Triglyceride reduction
Fat carrying capsules deliver triglyceride as well as cholesterol. When the capsules containing mostly triglyceride are overabundant in blood, the pancreas can become inflamed. The resultant illness, pancreatitis, can be very severe. Therefore, when blood triglyceride exceeds 500 mg/dl, treating LDL has to take a back seat to lowering triglycerides. Fatty acids are named partly by the presence (unsaturated) or absence (saturated) of kinks in their tail and where the kinks are located. If a kink is found three places from last (omega) carbon atom of the fatty acid, it is an Omega-3 fatty acid.
DHA and EPA are the key components to fish oils
Cold, salt-water fish caught fresh, not farmed, are common sources of Omega-3 fatty acids. Docosahexaenoic Acid (DHA) and Eicosapentaenoic acid (EPA) are the two most useful influences on blood concentration of triglycerides. Fish oil supplements are effective when more than 1000 mg/d of DHA and EPA are supplemented to the diet.
The fibrates are the most common pharmacologic choice to lower triglyceride. Only Fenofibrate or Fenofibric acid should be used in conjunction with a statin drug.
Antioxidants
Antioxidants are the cell’s version of protective clothing. Cells are constantly generating very small molecules called radicals while harvesting energy, for defense and for rudimentary communication. Radicals modify or divide other molecules without the help of enzymes. When radicals are produced in the course of harvesting energy, they may be cast off like sparks from a flame. The cell must protect itself from injury. Antioxidants are that protection.
Antioxidants have a time and a place. With CAD, we just don’t know what time and which place.
Radicals are involved in several processes believed to be important in the development and progression of CAD. As part of a communication network, oxygen-based radicals shift the cell’s general mood toward inflammation and clotting. Although these effects are undesirable in the arteries, antioxidants are unlikely to disrupt intentional communication inside of a cell. Radicals can affect LDL to make it more irritating to the arteries. Antioxidant supplements may protect LDL from this type of change. The better means of keeping LDL from becoming tarnished as it lingers in the wall of an artery is to lower the blood levels so much that it does not get trapped there in the first place.
Conclusion
The hardest recommendation to follow for prevention of heart attack is also probably the most important: eat less and exercise more. Even following a perfect lifestyle, some of us inherit a predilection to arterial decay that requires the assistance of medicines to reasonably lower our risk. The major question each of us has is, “Am I one of those people?” The answer is probably yes if,
You have diabetes.
You have an LDL cholesterol over 190 mg/dl.
You have already had a heart attack, stroke or peripheral artery disease.
A decision to take medicines after a heart attack is fairly straightforward. The natural course of disease without medicines is more dangerous than concerns for medicine side effects. Without such intimidation, the decision is difficult and very personal. A host of helpful tools can use your age and risk factors to calculate your risk of heart attack in the next ten years. However, no tool is more useful than sitting down with your physician who can put that risk into context and help you decide that medicine is warranted.